Public health epidemiologists have been dining out on the smoking-lung cancer link since the 1950s. They're not going to find anything as big as that again and the trophy cupboard has been fairly empty ever since.
'Public health' activists have been dining out on the tobacco industry's 'merchants of doubt' campaign since the 1990s and are eager to tar every industry of which they disapprove with the same brush.
The latest study is no exception. The gist of it is that the tobacco industry circa 1950-1980 put forward 'alternative causation arguments' to cast doubt over the smoking-lung cancer association. Indeed they did. There was talk of sulphur in matches being the real problem. Hans Eysenck suggested that the personality traits which led people to smoke also happened to increase the risk of developing cancer.
This was all obviously nonsense and we can laugh about it now. Petticrew's theory is that the same thing is going on today with regards to sugary drinks and alcohol. To get to the bottom of this, he and his chums conducted an online survey - the gold standard for 'public health' research these days - and gauged people's reactions to a series of statements.
They were subsequently presented with a short, anonymized, paragraph containing either an alternative causation argument about a particular harm obtained from one of the four industry-sponsored sources (randomly selected from examples from either the fossil fuels, smoking, alcohol, or sugar sweetened beverages industries), or information from an independent scientific or non-governmental agency.
Respondents were then asked about their certainty about the risk of the
specific harm from that product (certain it does increase risk,
uncertain it increases risk, certain it doesn't increase risk).
The idea was to see whether the industry's filthy lies would outweigh the impartial truth in the mind's of ordinary folk. Alas, they did.
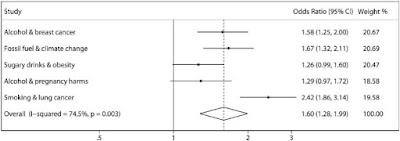
Overall, (i.e. grouping all industries together) industry-sponsored uncertainty messages significantly increased the odds of uncertainty, or false certainty, by 60%, compared to independent sources of information (Summary OR 1·60, 95% CI 1·28–1·99) (see Fig. 1 and Table 2).
It seems that about seven per cent of participants went from being certain to uncertain when presented with the 'industry text'. Weirdly, it seems that the biggest effect was found when people were presented with ancient statements from the tobacco industry, albeit from a lower (but still surprisingly high) base.
What kind of statements are we talking about? This is where it gets interesting. The authors don't include them in the study but they can be found in a ropey Word document in the supplementary material. For alcohol, the first statement from 'an independent scientific or non-governmental agency' is this...
"Alcohol is a Group 1 Carcinogen.
Like Tobacco." (Balance North East)
http://www.balancenortheast.co.uk/our-campaigns/alcohol-and-cancer/
Balance North East is an anti-alcohol pressure group entirely funded by the taxpayer. It is questionable whether it is 'independent' (from whom?) or 'non-governmental'. Either way, it has an incentive to portray alcohol in the worst possible light to drive support for its various campaigns, which include minimum pricing and advertising bans.
The claim about alcohol being a Group 1 carcinogen is true, but IARC's classifications are notoriously confusing to the general public since they are based on the strength of evidence rather than the magnitude of the risk. Processed meat is also a Group 1 carcinogen, but it is nothing like tobacco. As
Cancer Research UK explains...
While this may sound alarming, it’s important to remember that these groups show how confident IARC is that red and processed meat cause cancer, not how many cancer cases they cause, as we wrote when we covered a previous IARC decision on diesel emissions, and interviewed one of our experts in the causes of cancer.
As
Professor David Phillips – a Cancer Research UK-funded carcinogen
expert from King’s College London – explains, “IARC does ‘hazard
identification’, not ‘risk assessment’.
“That sounds quite
technical, but what it means is that IARC isn’t in the business of
telling us how potent something is in causing cancer – only whether it
does so or not”, he says.
To take an analogy, think of banana
skins. They definitely can cause accidents, explains Phillips, but in
practice this doesn’t happen very often (unless you work in a banana
factory). And the sort of harm you can come to from slipping on a banana
skin isn’t generally as severe as, say, being in a car accident.
But
under a hazard identification system like IARC’s, ‘banana skins’ and
‘cars’ would come under the same category – they both definitely do
cause accidents.
So the first supposed statement of fact from an impartial organisation related to alcohol is not from an impartial organisation and is likely to mislead the vast majority of people. In the study, Balance North East's claim is juxtaposed with the following statement from - you guessed it! - DrinkAware.
"It's important to put the risks from drinking alcohol into context. There are many other factors that increase the risk of developing breast cancer, some of which we can't control, like:
- Age: you're more likely to develop it as you get older
- A family history of breast cancer
- Being tall
- A previous benign breast lump
However, in addition to alcohol, other lifestyle factors such as being overweight and smoking are thought to increase your risk of developing breast cancer." (Drinkaware, UK)
Again, this is all true. Is it misleading? Aside from the fact that smoking isn't actually a risk factor for breast cancer, I wouldn't say so. In any case, it needs to be put in the context of an entire webpage and a downloadable fact sheet which makes it very clear that "drinking alcohol increases your risk of breast cancer". This is hardly 'merchants of doubt' territory.
The next pairing of 'non-industry sponsored' and 'industry sponsored' texts is...
"The Chief Medical Officers advise:
Alcohol can cause cancer, including breast and colon cancers" (Warning msg from Hobin et al, 2020)
"Not all heavy drinkers get cancer as multiple risk factors are involved in the development of cancers including genetics and family history of cancer, age, environmental factors, and behavioural variables, as well as social determinants of health" (Drinkaware, UK)
This is not actually from DrinkAware. It is from the Australian equivalent, DrinkWise. The same webpage says 'Excessive drinking can increase the risk of developing colon cancer' and 'Studies indicate a relationship between alcohol consumption and developing breast cancer'. Hardly the stuff of a hardcore denier.
It seems that Petticrew's beef is that DrinkAware and DrinkWise acknowledge that alcohol is not the only cause of cancer. This is obviously true. Alcohol causes only a small minority of cancers. If the aim is to educate the general public, the quotes from DrinkAware and DrinkWise are more informative than "Alcohol is a Group 1 Carcinogen.
Like Tobacco."
Some may disagree, but everyone should be able to agree that these 'industry-sponsored' organisations are not putting forward an 'alternative causation argument'. An alternative causation argument would be something like this:
Some studies have found a link between alcohol and cancer, but correlation doesn't equal causation and the statistical association may be due to factors such as X, Y and Z.
That is what the tobacco industry and its supporters did in the twentieth century. It is not what DrinkAware are doing. Pointing out that not every drinker gets cancer and listing some other causes of cancer is not an alternative causation argument. It is the truth and it is quite useful since most people would like to know what risks they face in life.
The next pairing takes a quote from Alcohol Concern - a defunct anti-alcohol pressure group - and the International Alliance for Responsible Drinking, an industry-funded body.
"For some cancers, any amount of alcohol increases the risk. For other types of cancer, the risk only increases after drinking two or three drinks per day – around 26 to 35 units per week.
Any amount of alcohol increases the risk of:
- Mouth cancer
- Upper throat and voice box cancer
- Food pipe (oesophagus) cancer
- Breast cancer" (quote from Alcohol Concern information on alcohol and cancer (now Alcohol Change https://alcoholchange.org.uk/alcohol-facts/fact-sheets/alcohol-and-cancer)
“Breast cancer is the leading cancer among women, and is associated with a large number of individual risk factors. Research has shown that breast cancer risk is associated with family history and hormonal and reproductive factors. Increased risk has been reported with hormone replacement therapy, but varies by the type of breast cancer (ductal, lobular, or mixed). Similarly, risk associated with other reproductive factors, such as age at menarche or breastfeeding, have been shown to differ by cancer subtypes. According to IARC, cancer of the female breast is causally associated with the consumption of alcohol beverages." (IARD, global)
In this instance, the 'industry-sponsored' message is more factual than the 'non-industry' message. The idea that
light drinking increases the risk of breast cancer is actually pretty shaky. The same is true of
laryngeal ('throat box') cancer. Meanwhile, the IARD statement is factually correct. It's difficult to see what Petticrew's problem with a sentence like 'According to IARC, cancer of the female breast is causally associated with the consumption of alcohol beverages' could be. Presumably he is upset because they mention other risk factors. It is understandable that a temperance pressure group wouldn't want to mention other risk factors, but it hardly seems unreasonable to do so.
The authors then move on to drinking in pregnancy with examples such as this:
If you are pregnant or planning a pregnancy, the safest approach is not to drink alcohol at all, to keep risks to your baby to a minimum.
(UK Chief Medical Officer Guidelines, UK)
https://www.gov.uk/government/publications/alcohol-consumption-advice-on-low-risk-drinking
There is confusion about how much
one can safely drink during pregnancy.
We know very clearly that excessive
amounts, either in isolated binge drinking or in prolonged drinking, are very harmful.
What we don’t know for sure is the lowest possible level that you can drink safely. We therefore say, for that reason, the safest possible thing that you can do is to not drink at all during pregnancy or while you’re breastfeeding.
(Drinkwise, Australia)
It is certainly true that there is 'confusion about how much
one can safely drink during pregnancy'. It is likely that there is a 'safe level' but it would be unethical to run a randomised controlled trial to establish what it is. In the absence of firm data, total abstinence is clearly the risk-free option. And that is exactly what DrinkWise recommends! Presumably Petticrew included this quote because it mentions uncertainty, but the uncertainty is very real.
They then move on to sugary drinks.
“Children who consume higher amounts of sugary drinks have a 55% greater chance of being overweight or obese compared to those who consume less [sic] sugary drinks." (American Heart Assn: (https://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_474846.pdf)
"Obesity is a complex problem that is influenced by many factors, most importantly diet, exercise and genetics. … The key to living a healthy lifestyle is to incorporate a balanced, healthy diet that balances calories consumed and calories burned through activity and exercise." (American Beverage Institute, sourced from Lim et al, 2019)
The 'impartial' commentators here are citing one
meta-analysis. Other meta-analyses have been published which find no such effect (see
here and
here). This suggests a large degree of genuine uncertainty. Meanwhile, the 'industry-sponsored' commentators make a statement of fact that is so uncontroversial I am at a loss to see why it is included by Petticrew et al.
“Excessive consumption of sugar is one factor promoting overweight and obesity. In 2013, about 37% of men and 38% of women worldwide were overweight or obese. Excess weight increases the risk of non-communicable diseases, including some cancers”. (NCD Alliance https://ncdalliance.org/sites/default/files/resource_files/Curbing-Global-Sugar-Consumption.pdf)
"Obesity is complex and there can be many causes. These include eating more kilojoules than your body uses, inactivity, genetics, conveniences linked to modern living, and socio-economic factors. For many, too much energy or kilojoules consumed from any source, including sugars, contributes to weight gain. For sugars and obesity, the research continues to show no direct causal relationship, outside of the contribution to energy intake." (Sugar Nutrition Research Centre https://www.sugarnutritionresource.org/sugar-health/sugar-and-obesity)
I can't see much of a difference between these two statements. They are both factually correct and uncontroversial.
It would be tedious to give more examples. The most that can be said is that the 'industry-sponsored' messages sometimes have a slightly different emphasis than the messages from campaign groups. Specifically, the 'industry-sponsored' messages - or, more precisely, the messages that have been handpicked by Petticrew and friends - are more likely to mention other risk factors than the messages from 'non-industry sponsored' organisations.
Even this is debatable. If you look at the NHS's webpage about breast cancer, it only briefly mentions alcohol at the bottom of its list of risk factors. It is the same list of risk factors given by DrinkAware in the quote above which is supposedly 'misinformation'.
The study concludes with a little rant and a call to action.
The potency of this misinformation is of concern in part because
exposure to it is widespread. Compared to the tobacco industry, which
has now been prevented from many forms of public engagement, the fossil
fuel, alcohol, and sugar sweetened beverage industries have far wider
access to the public as conveyors of misinformation, including by
funding charities with the express purpose of communicating on product
harms to the general public, as well as to children and young people
through schools.
He is talking about DrinkAware, of course. Did I mention that he is obsessed?
By way of
example, Drinkaware, an alcohol-industry-sponsored charity in the UK,
whose misinformation is used in two of our examples, is named on most
alcohol-related advertising labels, posters and adverts, and its
website, from which the information used in this study was obtained,
received over 10 million unique visitors in 2018 (DrinkAware. Impact
Report, 2018). Just as “the dose makes the poison”, the impact of these
messages is a function of both their potency, and their breadth of
exposure.
DrinkAware need to take out a restraining order against this guy.
Dialing the madness up to 11 in the conclusion, the authors suggest that charities such as DrinkAware should be banned from talking about health risks, presumably by law.
.. This evidence brings into question whether manufacturers of harmful
products and charities with funding from such manufacturers should be
permitted to communicate about health risks with the public.
And there is a clue as to what their next studies are going to be about.
.. Future research could focus on messages regarding other harmful products such as gambling or vaping.
Something to look forward to.
And, in case you were worried, the researchers took their duty of care very seriously. No one was hurt as a result of this experiment.
At the end of the survey respondents were presented with accurate
independent (non-industry) information, and a link to a trusted source
(e.g., the relevant NHS England information or other independent
source). Each respondent was exposed to misinformation from only one
industry.
That's a relief.